
Psychosocial risk assessment for Queensland employers

Psychosocial hazards are not a feel‑good wellbeing initiative; they are recognised work health and safety (WHS) hazards. Queensland’s Work Health and Safety Act 2011 defines health as “physical and psychological health” and requires persons conducting a business or undertaking (PCBUs) to ensure, so far as reasonably practicable, the health and safety of workers. This duty includes consulting with workers when identifying hazards and deciding how to control risks. Under the WHS Regulation, psychosocial hazards are aspects of work design, the work environment, plant or workplace interactions that can cause psychological harm even when physical harm is absent. Queensland’s Managing the risk of psychosocial hazards at work Code of Practice 2022 lists common hazards such as high job demands, low control, poor support, violence and aggression, bullying and harassment and emphasises that hazards often interact or accumulate over time. Because Queensland has no single “replacement” for the People at Work survey, WorkSafe recommends using risk assessment tools aligned to the 14 hazard categories in the code and treating surveys as just one of several evidence sources.
This article provides a non‑commercial, evidence‑based methodology for psychosocial risk management. It is written for Queensland PCBUs and officers who need a process that aligns with the WHS Act, the WHS Regulation, the 2022 code and international standards (ISO 45001 and ISO 45003). All footnotes link to primary sources and evidence.
Why psychosocial risk is a legal and business imperative
· Legal clarity: The WHS Act requires PCBUs to eliminate or minimise risks as far as reasonably practicable, and officers must exercise due diligence by ensuring the PCBU has resources and processes to control risks. Psychosocial hazards are included in these duties, and failure to manage them can attract the same penalties as physical hazards.
· Psychosocial hazard definition: Under the WHS Regulation, psychosocial hazards arise from work design or management, the work environment, plant, or workplace interactions/behaviours and can cause psychological harm. Examples include unreasonable job demands, low job control, poor support, lack of role clarity, poor change management, inadequate reward and recognition, poor organisational justice, remote/isolated work, traumatic events, violence and aggression, bullying and harassment.
· National context: The Commonwealth Managing Psychosocial Hazards at Work Code of Practice 2024 expands the list to 17 hazards, adding explicit references to job insecurity, fatigue and intrusive surveillance. Multi‑jurisdictional employers should use this broader taxonomy as a completeness check.
· Economic costs: Safe Work Australia data show that mental health conditions accounted for about 9 % of serious workers’ compensation claims in 2021‑22, up nearly 37 % since 2017‑18, with work pressure, harassment/bullying and violence among the leading contributors. These claims have a median cost more than three times higher than other serious injury claims.
· Evidence for organisational controls: Systematic reviews demonstrate moderate to strong evidence that organisational‑level interventions—changes to work design, staffing, workload and organisational processes—can improve psychosocial work environments and reduce burnout. In other words, treating psychosocial hazards like “engagement” issues is ineffective; the focus must be on design and systems.
Aligning with ISO 45001 and ISO 45003
ISO 45001 provides a framework for occupational health and safety management systems based on the Plan–Do–Check–Act cycle[9]. ISO 45003 offers specific guidance for managing psychosocial risk within an ISO 45001 system and stresses the need to protect and promote both physical and psychological health. The Queensland methodology described below aligns with this framework: it uses a systematic cycle, integrates psychosocial risk into existing WHS processes and emphasises continual improvement.
Step‑by‑step psychosocial risk management methodology
1 – Establish scope, governance and “what good looks like”
· Define the boundary: Decide whether the assessment covers the whole organisation, a business unit, high‑risk roles or specific sites. Include contractors, labour‑hire and volunteers where relevant; the WHS Act applies broadly to anyone carrying out work.
· Set governance: Appoint an executive sponsor (accountable for resourcing and authorising controls), a WHS lead (method owner), operational leaders (responsible for implementing controls), HR/IR support and worker representatives/health and safety representatives. Officers’ due‑diligence obligations mean they must ensure resources and processes exist and are used.
· Articulate success: Clarify that the objective is to identify hazards, assess exposure and implement higher‑order controls, not to gauge “happiness” or run a tick‑box survey.
2 – Identify hazards using the Queensland and Commonwealth taxonomies
Use the Regulation’s organising frame—work design/management, work environment, plant, and workplace interactions/behaviours—and map hazards to the Queensland code’s 14 categories. Cross‑check against the Commonwealth code’s additional hazards (job insecurity, fatigue, intrusive surveillance). Consider developing a “work map” by job family or function to systematically evaluate which hazards are reasonably foreseeable. Remember that hazards can interact or accumulate; for example, high demands combined with low support and exposure to customer aggression may produce greater harm than any hazard alone.
3 – Collect evidence from multiple sources
Queensland’s consultation duty requires sharing relevant information with workers, inviting their views and taking those views into account. To meet this duty and avoid bias, collect evidence from several sources:
· Surveys: Use open or licensed instruments that measure hazard exposures (job demands, control, support, etc.) rather than clinical symptoms. Survey at the level where controls can be implemented (team, role or site) and ensure anonymity through minimum group size thresholds. WorkSafe Queensland’s guidance notes that risk assessment tools aligned to the 14 hazards should replace purely engagement‑focused surveys.
· Focus groups/workshops: After surveys, conduct facilitated focus groups to explore “why” patterns exist and to co‑design controls. The UK Health and Safety Executive (HSE) Management Standards approach requires focus groups to validate survey data and develop action plans.
· Operational data: Review incident reports, complaint registers, bullying and harassment investigations, workers’ compensation claims and return‑to‑work data. Safe Work Australia notes that harassment/bullying and work pressure drive a high proportion of mental health claims.
· Absenteeism, turnover and exit interviews: Use these as corroborating evidence, recognising that they are influenced by labour market conditions. Observe patterns by location or role.
· Work design and observation: Analyse rosters, workload metrics, staffing ratios, role descriptions and change impacts. Walk through work processes to identify pinch points, supervision style and exposure to violence or aggression. These methods align with the Regulation’s requirement to consider work design, systems of work and workplace design when determining controls.
4 – Assess risk using likelihood, severity and exposure
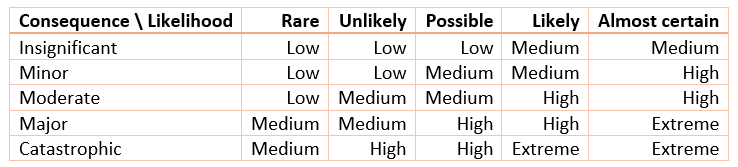
The WHS Regulation requires PCBUs to identify reasonably foreseeable hazards and to eliminate or minimise risks by considering the duration, frequency and severity of exposure, and how hazards interact[2]. A pragmatic psychosocial risk assessment model includes:
· Likelihood: Rare, unlikely, possible, likely or almost certain that harm will occur.
· Severity of harm: Credible worst‑case and most‑likely harm, including psychological and physical harm.
· Exposure: Frequency, duration and intensity of exposure, multiplied by the number of workers exposed.
· Interacting hazards: Identify combinations that amplify risk—e.g., high demands with low support and aggression exposure.
· Vulnerable groups: Consider workers who may face differential exposure (e.g., early‑career staff, culturally and linguistically diverse workers, remote workers). The Commonwealth code stresses that different groups may face different psychosocial hazards.
Apply these criteria to each identified hazard and record the outcome in a risk register. Use a 5×5 risk matrix for prioritisation but modify likelihood ratings upward if exposure is frequent, prolonged or severe or if multiple hazards interact. This reflects the Regulation’s emphasis on exposure and interaction.
5 – Prioritise risks and apply the “reasonably practicable” test
The Act defines “reasonably practicable” by weighing the likelihood of the risk occurring, the degree of harm, what is known about the hazard and controls, the availability and suitability of controls and the cost of implementing them (after assessing risk and controls)[1]. Prioritise:
· Hazards with both high severity and high exposure (e.g., frequent aggression or traumatic content).
· Hazards that affect many workers (e.g., workload, role clarity).
· Hazards known to drive compensation costs and poor return‑to‑work outcomes, such as harassment/bullying and work pressure.
Make prioritisation transparent and consult with workers about the rationale and proposed actions.
6 – Select controls using the hierarchy of controls
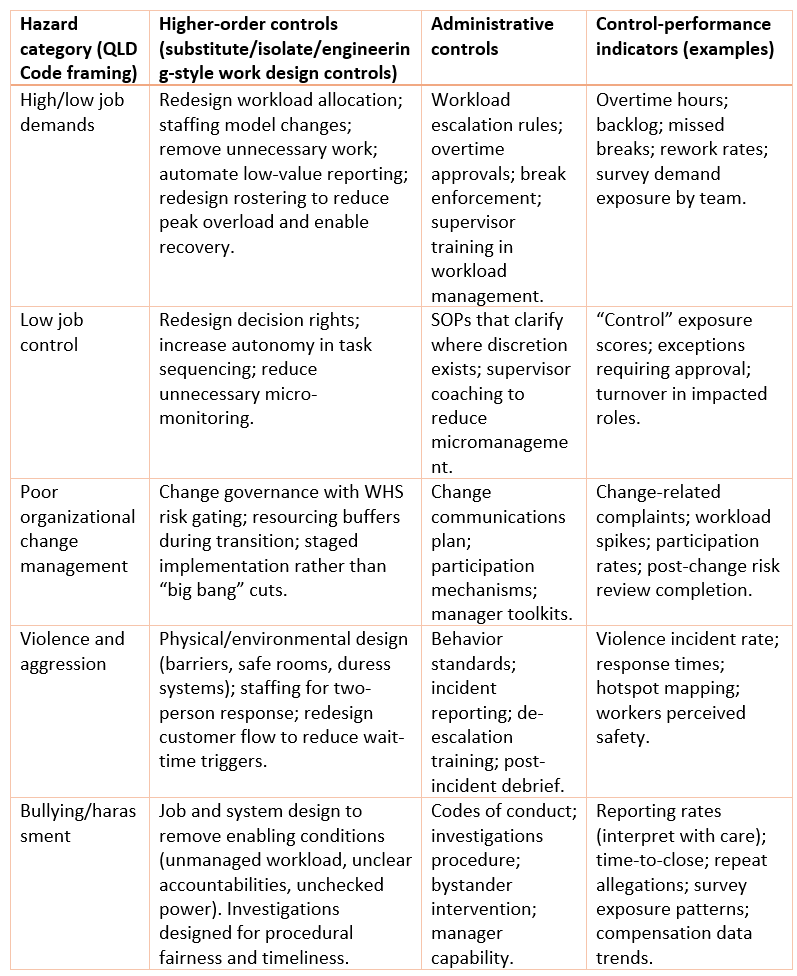
The hierarchy of controls applies to psychosocial hazards just as it does to physical hazards: eliminate the hazard or substitute/isolate/engineer it where reasonably practicable, then use administrative controls; personal protective equipment is a last resort. Higher‑order controls for psychosocial hazards often involve changes to work design, staffing models or physical environment. Evidence shows that organisational‑level interventions can improve psychosocial work environments and reduce burnout.
Below is a non‑exhaustive table linking common hazard categories to high‑order and administrative controls. Use it as a starting point and adapt through consultation.
7 – Plan implementation and document the risk assessment
The code and risk assessment tools recommend documenting hazards, evidence sources, risk ratings, existing controls, control adequacy, further controls, owners, monitoring approaches and review dates. Record consultation activities and outcomes so that inspectors and officers can verify compliance[3]. Without written records, PCBUs must still demonstrate compliance, which is difficult in practice.
8 – Monitor, verify and review controls
Under the Regulation, PCBUs must maintain and review control measures whenever there is an incident, consultation indicates the need, a significant change occurs or at regular intervals[2]. Build monitoring and verification into governance:
· Leading indicators: workload thresholds breached; aggression hotspot rates; change‑management risk gates completed; hazard exposure scores.
· Lagging indicators: serious mental health claim trends, absenteeism, turnover, time lost and compensation costs[6].
· Verification: internal audits, executive “walk‑arounds”, field verification and independent assurance to ensure controls are implemented and effective.
· Review triggers: incidents, complaints, organisational changes, consultation feedback or scheduled cycles (e.g., annual re‑assessment).
Evidence toolkit and measurement frameworks
A non‑commercial approach does not mean “guesswork.” Several open or licensed frameworks support psychosocial risk assessment. Choose an instrument that can be mapped to the Queensland hazard categories, produces outputs that drive control decisions and supports consultation.
· HSE Management Standards (UK): Focuses on six domains—demands, control, support, relationships, role and change—and includes a 35‑item Indicator Tool. The HSE emphasises combining survey data with focus groups to develop action plans. It does not cover all Queensland hazards (e.g., violence, bullying), so additional assessment is needed.
· COPSOQ III (Copenhagen Psychosocial Questionnaire): A broad, research‑based instrument covering multiple psychosocial domains; the questionnaire is available under a Creative Commons licence that prohibits commercial use and modifications. It offers rich constructs and psychometric robustness but requires careful implementation and mapping to local hazards.
· Guarding Minds at Work (Canada): Provides a survey and an eight‑step process aligned to the Canadian National Standard for Psychological Health and Safety; the tool is free to access and includes comparative reporting. Domains differ from the Queensland hazard taxonomy, and benchmarks are Canadian, so interpretation must consider context.
When designing your own survey, ensure each item maps to a hazard pathway (job demands, role clarity, organisational justice, etc.), avoid clinical screening questions, protect anonymity through minimum group sizes and commit to mixed methods (surveys plus qualitative follow‑up). Treat survey results as hypotheses requiring validation, not as final truth.
Implementation timeline and board reporting
For a single site or business unit, a typical initial cycle spans 12–16 weeks:
1. Weeks 1–2: Define scope, governance, consultation plan and hazard taxonomy mapping.
2. Weeks 3–6: Collect evidence (survey, operational data, focus groups).
3. Weeks 7–8: Conduct risk assessment workshops and develop a draft risk register.
4. Weeks 9–12: Design controls, assign owners and consult workers on proposed actions.
5. Weeks 13–16: Implement priority controls and establish monitoring indicators and review triggers.
For large or multi‑site organisations, stagger the roll‑out and adopt a quarterly monitoring and annual re‑assessment cadence. Officers should receive board‑level reports that highlight top risks, exposure patterns by hazard and work group, control implementation status, and leading and lagging indicators. Avoid “vanity metrics” like overall wellbeing scores; board reporting should focus on hazards, controls and assurance.
Governance, assurance and board reporting
Officers cannot “set and forget” psychosocial risk. Due diligence requires active steps: ensuring resources/processes exist and are used, ensuring information is received/considered/responded to, and ensuring compliance processes are implemented. This means psychosocial risk assessment must produce board-grade evidence: clear hazards, quantified exposure patterns, risk ratings, control decisions under the hierarchy, and verified implementation status.
Board reporting: what “good” looks like
A board psychosocial risk dashboard should avoid vanity metrics (“wellbeing score”) and focus on hazards, controls and verification, consistent with the WHS Regulation and Code logic. A minimal dashboard pack:
· Top psychosocial risks by residual risk rating, with control approach aligned to hierarchy of controls.
· Exposure patterns by hazard and work group (where anonymity thresholds met).
· Control implementation status (due dates, completion, verification checks).
· Leading indicators (e.g., workload thresholds breached; aggression hotspot rates; change risk gates completed).
· Lagging indicators (serious mental health claims trends; time lost; compensation cost; noting harassment/bullying and work pressure are major contributors nationally).
· Assurance statement from internal audit or external assurance against WHS Act/Reg/Code requirements.
Conclusion
Psychosocial hazards are WHS hazards that require the same structured risk management as physical hazards. Queensland law makes this explicit, and the 2022 Code of Practice provides detailed guidance on hazard categories and control expectations. By following a systematic, non‑commercial methodology—scope and governance, hazard identification, evidence collection, risk assessment, prioritisation, control selection, implementation planning and monitoring—PCBUs and officers can meet their legal duties, protect worker health and create psychologically safe workplaces. Incorporating evidence from open frameworks, international standards and peer‑reviewed research ensures that control decisions are defensible and effective.
References
Work Health and Safety Act 2011 (Qld).
https://www.legislation.qld.gov.au/view/whole/html/current/act-2011-018Work Health and Safety Regulation 2011 (Qld), including Division 11 Psychosocial Risks and Part 3.1 General Risk Management.
https://www.legislation.qld.gov.au/view/whole/html/inforce/current/sl-2011-0240Managing the Risk of Psychosocial Hazards at Work Code of Practice 2022 (Qld).
https://www.worksafe.qld.gov.au/__data/assets/pdf_file/0025/104857/managing-the-risk-of-psychosocial-hazards-at-work-code-of-practice.pdfWorkSafe Queensland. People at Work – Risk Assessment Guidance.
https://www.worksafe.qld.gov.au/safety-and-prevention/mental-health/people-at-workWork Health and Safety (Managing Psychosocial Hazards at Work) Code of Practice 2024 (Cth).
https://www.legislation.gov.au/F2024L01380ISO 45001:2018 Occupational Health and Safety Management Systems.
https://www.iso.org/standard/63787.htmlISO 45003:2021 Psychological Health and Safety at Work – Guidelines for Managing Psychosocial Risks.
https://www.iso.org/standard/64283.htmlStandards Australia. Guidance on ISO 45003 and psychosocial risk management.
https://www.standards.org.au/news/new-standards-document-to-help-manage-workplace-psychosocial-riskSafe Work Australia (2024). Psychological Health and Safety in the Workplace – Data Report.
https://data.safeworkaustralia.gov.au/sites/default/files/2024-02/Psychological-health-in-the-workplace_Report_February2024.pdfHSE (UK). Management Standards for Work-Related Stress.
https://www.hse.gov.uk/stress/standards/overview.htmCOPSOQ International Network. Licence Guidelines and Questionnaire.
https://www.copsoq-network.org/licence-guidelines-and-questionnaireGuarding Minds at Work. Psychological Health and Safety Framework.
https://www.guardingmindsatwork.ca/Madsen, I.E.H. et al. (2021). Psychosocial work exposures and mental disorders – systematic review.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8504166/Montano, D. et al. (2024). Organisational-level interventions and psychosocial outcomes – systematic overview.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10713994/LaMontagne, A.D. et al. (2014). Integrated approaches to workplace mental health.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4024273/